Denver Sacroiliac Joint Dysfunction/Sacroiliitis Specialists
Understanding Sacroiliac Joint Dysfunction
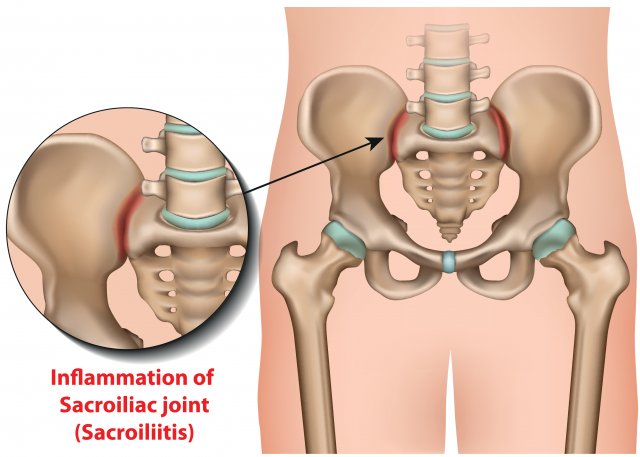
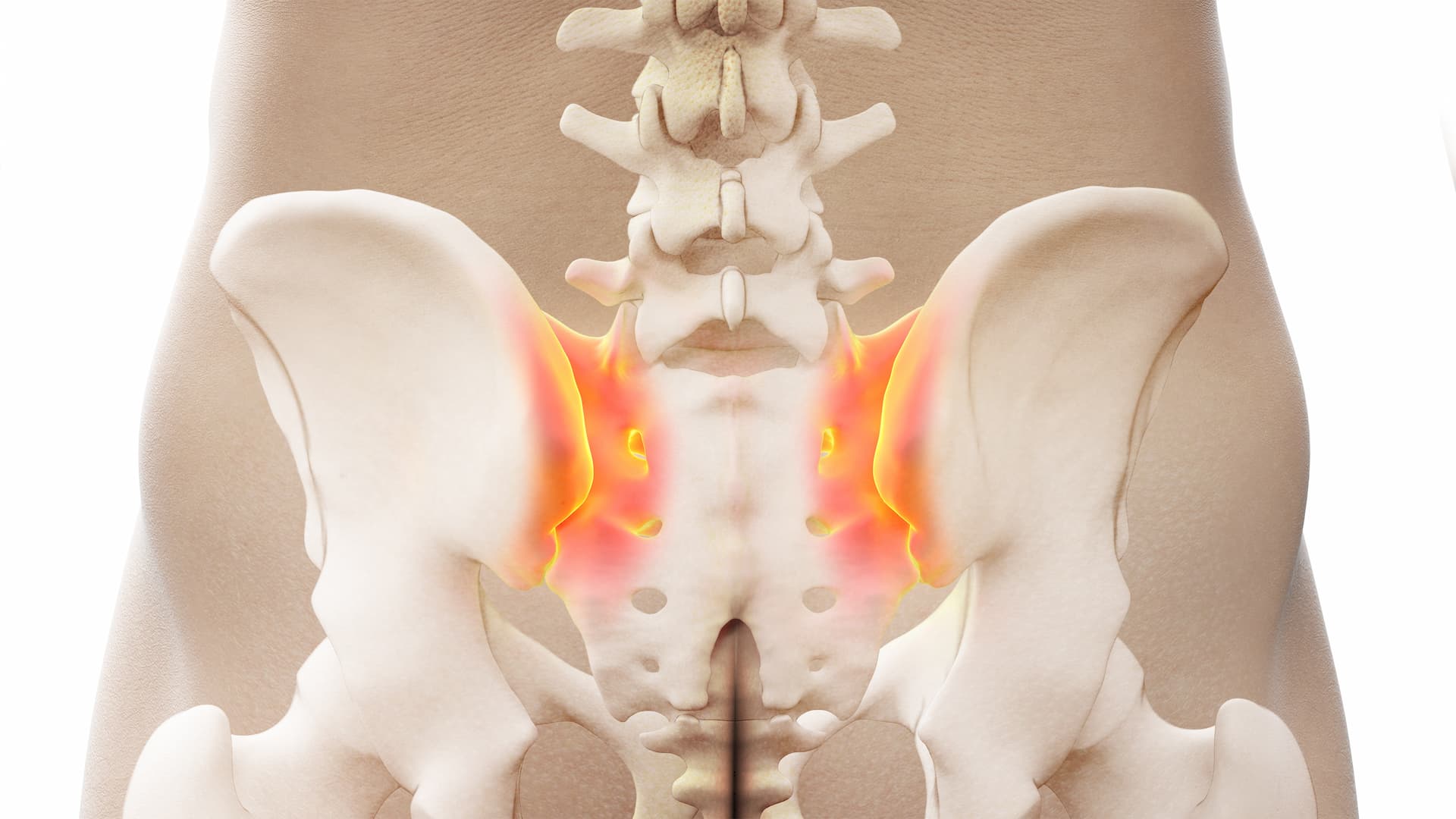
Sacroiliac joint (SIJ) dysfunction is pain stemming from the sacroiliac joint, which connects the iliac crests to the sacrum. SIJ dysfunction is often associated with either hypermobility or hypomobility of the joint. The SIJ is a 75% synovial joint with the remainder being fibrocartilaginous in nature. The superior aspect of the joint is often fused while the lower portion is more typical of a true synovial joint. It is innervated by lumbar and sacral dorsal rami (lumbar medial branch and sacral lateral branch nerves) as well as the lumbosacral plexus and superior gluteal nerves.
Diagnosis
SIJ dysfunction can be difficult to diagnose especially as it mimics other sources of pain. Typically, SIJ pain is described as low back and buttock pain as well as radiating pain into the upper leg and groin. Up to 30% of patients with low back pain actually have been found to have pain arising from the SIJ. Patients may report pain with position changes such as standing from a seated position or sitting on a hard surface. Relief with lying down or walking may be noted. There are many provocative maneuvers to help in the diagnosis such as FABER, Gaenslen’s, and thigh thrust tests. Overall these have shown to have a low sensitivity and specificity. Although Imaging modalities may be employed (radiographs, CT, MRI scans) in general these are not especially helpful as few abnormalities may be seen. Findings to look for include joint space narrowing and/or sclerosis of the SIJ. The most definitive evaluation is image guided injections of the SIJ with local anesthetic only. Greater than 75% relief would be diagnostic for SIJ dysfunction.
Comprehensive SIJ Dysfunction Treatment Options in Denver
Treatment starts with conservative care including physical therapy modalities and anti-inflammatory medications. Manipulative therapies have also been described. If these options fail, injections can not only provide diagnostic information but also therapeutic relief. Injection options include image guided SIJ intra-articular steroid injections and/or blocks of the L5 medial branch + sacral lateral branch nerves. If indicated radiofrequency ablation of these nerves can be done and provide longer term relief. Percutaneous SIJ fusion is also a new non-surgical option. Finally, if these modalities fail the next step would be evaluation for surgical treatment.
At MD Pain, we take a comprehensive approach to SI joint dysfunction, evaluating both upper and lower body mechanics to ensure a proper diagnosis. Our specialists utilize targeted sacroiliac joint injections and SI joint injections to relieve pain and provide lasting pain relief for patients experiencing SI joint pain. By combining these advanced treatments with personalized care and lifestyle guidance, we help patients restore mobility, improve daily function, and effectively relieve pain associated with SI joint issues.
Personalized Sacroiliac Joint Care Near You in Denver
MD Pain specializes in sacroiliac joint dysfunction treatment for patients in the Denver Metro and Colorado Springs areas. Our team of experienced pain specialists takes the time to evaluate your unique pain patterns, activity levels, and medical history. By combining advanced diagnostics with proven treatment strategies, we help patients regain mobility, reduce discomfort, and return to their daily routines.
Living with Sacroiliac Joint Dysfunction: Tips for Daily Life
Managing sacroiliac joint pain involves more than just medical treatments. MD Pain offers practical guidance to help patients manage discomfort and maintain daily activity:
- Avoid prolonged sitting on hard surfaces and alternate positions regularly
- Use supportive seating or cushions when sitting
- Incorporate low-impact exercises like swimming or walking to strengthen core and hip muscles
- Practice gentle stretching and mobility routines recommended by your provider
- Track pain patterns to better inform treatment decisions
Combining these strategies with professional care can significantly improve quality of life for those living with SIJ dysfunction.
References:
Ou-Yang D, et al. Diagnosis and Management of Sacroiliac Joint Dysfunction. Journal of Bone and Joint Surgery. 2017:99:2027-36.
Zelle B, et al. Sacoiliac Joint Dysfunction. Evaluation and Management. Clinical Journal of Pain. Oct 2005;21(5):446-455.
Your Questions About SIJ Dysfunction Answered
What causes sacroiliac joint dysfunction?
Sacroiliac joint pain can result from hypermobility, hypomobility, trauma, or degenerative changes in the joint. MD Pain evaluates each patient’s history, imaging, and response to diagnostic injections to determine the exact cause of discomfort and develop a precise treatment plan.
How is SIJ dysfunction diagnosed?
Diagnosis can be challenging, as SIJ pain often mimics other types of low back or hip pain. MD Pain uses a combination of physical examinations, provocative maneuvers, imaging studies, and image-guided injections to accurately identify sacroiliac joint dysfunction.
What treatment options are available at MD Pain?
Our Denver specialists provide a full spectrum of care, from conservative therapies and anti-inflammatory strategies to advanced interventions such as nerve blocks, radiofrequency ablation, and minimally invasive fusion procedures. Every plan is personalized for the patient’s condition and lifestyle.
Is sacroiliac joint pain permanent?
With appropriate care, many patients experience significant relief and improved function. MD Pain emphasizes early intervention, proper exercises, and targeted therapies to reduce pain and prevent recurrence, helping patients return to normal activities.
Why choose MD Pain for SIJ dysfunction treatment in Denver?
MD Pain has years of experience treating sacroiliac joint dysfunction in the Denver Metro and Colorado Springs areas. Our board-certified physicians and pain specialists combine expertise, compassion, and advanced treatments to provide effective, long-lasting relief near you.